


By Michael Useem and Stephen K. Klasko, M.D.1
The search committee for a new chief executive of the Jefferson health system in 2013 had narrowed the field to three candidates. Each qualified, all respected, the recruitment ought not go wrong whoever the finalist.
Yet as an afterthought, the search committee retrieved an unlikely CV for an outlier named Stephen Klasko, an obstetrician-gynecologist serving as dean of a Florida medical school – and co-author of this article. Like the frontrunners, he came with many of the givens for running a healthcare enterprise, including thinking strategically, communicating persuasively, and acting decisively. Solid though not standing out on any of those traditional markers, in the view of the search committee, Klasko had so far ranked, in his own telling, “as 16th of 15 candidates by the traditional metrics of operations, focus, and discipline.”2
Yet in other ways Klasko did stand out: restless, determined, even a flame thrower when it came to righting the fixable wrongs of organized medicine. His “no limits” mindset displayed a readiness for heretical actions and confidence in their long-term payoffs even if others disparaged such actions now. Acknowledging that there can be “a fine line between crazy and visionary,” if “you are willing to be called crazy,” he told himself, “people will call you a visionary once you are successful.”
A Candidate for Good and Trying Times
Though Klasko’s lesser operational credentials – he had never run a hospital let alone a health system or an entire university – initially placed him below the top tier of the applicant pool, his leadership capacities were actually more comprehensive than those of many of the otherwise more highly ranked candidates if wholesale change was also to become a priority for Jefferson.
As of the time of the search, though change was desired it was not the modus operandi at Jefferson, which had been living with interim leadership for more than a year.
Still, Jefferson was coming off a successful year as it searched for the new CEO in 2103, and did it really need a new executive with an augmented repertoire, dedicated to not only running the institution but also transforming it? In patient readmissions, a benchmark for the U.S. Centers for Medicare and Medicaid Services, Jefferson rated well. And so too did the hospital’s annual revenue. For sustaining Jefferson’s prosperous times, then, the original finalists understandably ranked higher on the list.

Yet in the evolving view of the search committee, the world in which Jefferson operated did not appear all that right and secure. A seasoned hand and a maverick with an ability to steady the rudder in normal times but who could also redirect it in trying times might thus be a superior choice. All told, Klasko seemed better than the initially higher-ranking candidates to fit the expanded search criteria for not only guiding the current operations but also for remedying them.
Redressing Jefferson’s management seemed increasingly imperative. Growing shortfalls in healthcare both nationally and locally included soaring costs, unequal services, and the troublesome irony of life spans declining in an ever more affluent nation. In 2013, the number of hospitals and beds had been shrinking nationally, and Jefferson itself had suffered a seven-percent admissions decline. In the diagnosis of the president of the American Medical Association, America’s public health system had become “critically ill.” And possibly ahead: a viral menace that could overwhelm intensive care units and hospital services worldwide, including those of Jefferson, if they stuck to business as usual.3
In what would have seemed implausible at the beginning of the search, the Jefferson search committee turned to the “upset” candidate, concluding that Klasko actually came with a more complete template for running the health system both as it was and as it could and should be. He was strategic but also iconoclastic. The committee believed he could deliver both the conventional and the exceptional, bringing what has always been essential for leading health services but also what had become critical for more turbulent times.4
“Jefferson was in a position of stability, and we were in good financial shape,” recalled David Binswanger, co-chair of the search committee, “but we also had to get our feet out of the mud. We were all stuck and we wanted somebody who could make a change.” The existential question in front of the search committee, in the words of its other co-chair, William Landman: “Do we change incrementally or transformationally?” And if the latter, Klasko became the favored candidate. They believed he could simultaneously run the enterprise and transmute it. To manage Jefferson and course-correct it, Klasko emerged as the leadership-plus candidate.5
Leadership Plus
Most of the traditional capabilities for running a health provider are a recognized part of the leadership canon, but the additional principles for navigating a more disparate and disruptive era are less well established, and they are the primary focus here. To identify those additional capacities, we delve into the experience of this health system with a rarely combined insider’s experience and outsider’s appraisal. Drawing them together as factually as possible, we seek to identify a more complete leadership roadmap for those called to lead through both prosperous and transformative times.6
For this purpose, we focus on what consulting-firm McKinsey & Co. has termed “big bets” – those sharp-edged actions that executives and directors take from time to time that can derail a firm if taken wrongly but accelerate it if taken rightly. It is at such points that enterprise leadership, we believe, can often be best parsed for its essential qualities.7
For those looking to lead their company well but also to prepare it for restructuring or even crisis response, whether facing a moment of innovation or a global pandemic, our main message here: We want not only to double-down on the traditional leadership capacities that have served us well in normal times but also to incorporate additional leadership capacities that become especially critical for mapping our way through trying times.
Running and Reforming for Performance
Jefferson installed Klasko as its new chief executive on June 20, 2013, casting its lot not only with a restless change maker but one who could bring together a team to combat the inevitable inertia at a traditional academic medical center. In doing so, the board bet that one person with the requisite blend of leadership capabilities could both run and transform the enterprise.
It was a weighty wager. Was the new CEO’s abiding determination enough to transmute the enterprise in fact? Could one individual, however resolute, actually alter Jefferson’s traditional pathways for patient care, teaching, innovation and philanthropy? And would the new CEO at the same time be able to keep the current engine running?
The dual leadership agenda of sustaining the on-going operations while building the new was certainly at the center of Klasko’s personal commitment when he arrived. “How do you run a large complex organization,” he asked himself on taking the reins, while also “turning it 180 degrees around?” To achieve both, he advocated, “you have to think what’s possible” a decade forward and then work backwards,” bringing that future into the present.” It would be treacherous, of course, but “the biggest risk,” he warned, was that Jefferson would neither prosper nor transform itself ahead of the growing threats to organized medicine. He personally savored the perils of achieving both. “What turns me on,” he confessed, “is risky impact,” high-stakes actions to both sustain and modernize the model.
Forceful resistance was sure to be expected from the ranks, Klasko acknowledged, casting doubt on the transformative half. Jefferson carried nearly two centuries of accumulated wisdom and established tradition since its founding in 1824. Many of its incumbents had been directing the institution for years, their sweat equity and personal identity deeply embedded in its present configuration. The name of Thomas Jefferson, an historic symbol of steadfastness, greeted all coming through the front door.
None of that natural inertia, however, proved sufficient to thwart the current and transformative agendas of the new chief. Topping Klasko’s metamorphic plan: consolidating a host of health providers in the Philadelphia region on the premise that the resulting scale would generate better patient outcomes – a key objective – as he spread administrative efficiencies and health practices across providers.
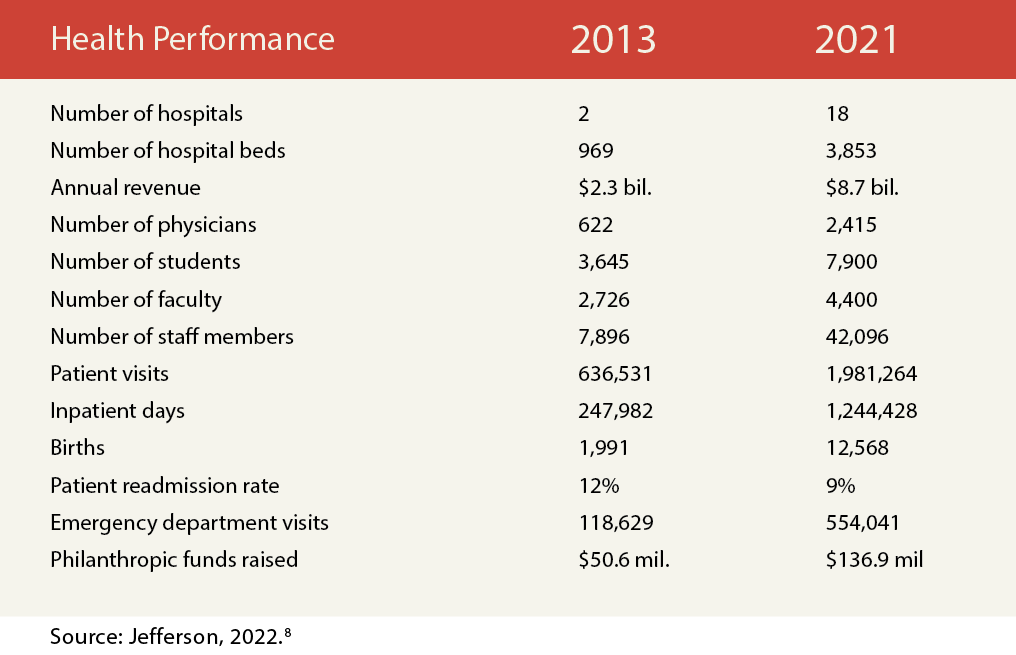
Assorted metrics paint a picture of wholesale conversion. Klasko combined several governing boards, allowing him to merge Thomas Jefferson University with Philadelphia University (a fashion design and architecture university) to increase student enrollment from 3,645 to 7,900. He added 16 hospitals to a starting slate of two, and increased Jefferson’s annual revenue by a factor of 3.8, from $2.3 billion to $8.7 billion. On his arrival in 2013, the system employed 622 physicians and 2,726 faculty; by 2021, its rolls had grown to 2,415 physicians and 4,400 faculty. At his start, Jefferson drew 636,531 patient visits annually, but nearly two million eight years later (Table 1).
TABLE 1. Metrics for Jefferson’s Health-Related Performance, 2013 and 2021
Klasko’s moves were initially met with public skepticism, but they resulted in Jefferson becoming the largest health provider in the Philadelphia region, the country’s seventh largest metropolitan statistical area.9
The search committee had selected Klasko over his fifteen competitors on the premise that he would apply the leadership repertoire required for transformative change while sustaining the original enterprise at the same time. At the center of the leadership repertoire for the first was his own belief that he could take personal charge and execute the change, and that a single but determined individual with the requisite capabilities could make a radical difference. At the center of the leadership repertoire for the second was his belief that he had the leadership precepts to operate the enterprise well however it might be changed.10
Jefferson’s first big bet, then, was that its new CEO had the commitment and capabilities to transform Jefferson’s direction while sustaining its ongoing performance. In the framing of London Business School professor Herminia Ibarra, who studied a number of managers taking on company leadership, Klasko had accepted and executed the search committee’s calling. He embraced the leadership identity of being both a steady hand and a change agent. And he enacted that dual identity, we shall see, through two leadership add-ons, big bets themselves: reducing risk and redefining benchmarks. They came to be the + in Klasko’s leadership-plus, his transformative tenets in addition to his traditional teachings.11
Reducing Risk
A first add-on feature of Klasko’s leadership agenda came from his decision to ready the institution for the risks ahead, strengthening its resilience and steadying its hand for the setbacks or even calamities that could strike in the future. Foreseeing the time ahead and bringing its implications into the present proved vital, as we will see in Jefferson’s early readiness to face the coronavirus crisis and to build-out telemedicine before it would be needed.
As Klasko’s remake of Jefferson was gathering steam after six years in the chair, the city of Wuhan in central China reported a peculiar pneumonia-like virus in late 2019. Soon, the novel infection was spreading rapidly, asymptomatically, and internationally, leaping silently from one hot zone to another, some a continent away. By the end of 2020, the new coronavirus had infected more than 80 million people worldwide and killed more than 350,000 in the U.S alone. By the end of 2021, American fatalities exceeded 800,000.
For avoiding the worst in his health complex, however, Klasko’s team had already sought to strengthen Jefferson’s capacity to see coming calamities, anticipating their implications for healthcare when preemptive steps could still be taken. The private sector’s globalization had facilitated just that, and Klasko pushed his hospital to do the same, believing that expanding abroad would prove propitious for care at home, breaking the “not-invented-here” syndrome that domestic institutions sometime embraced in their isolation. To that end, Klasko brought in a transplant surgeon and former mayor of Rome, Dr. Ignazio Marino, and created the Jefferson Italy Center in Rome, a partnership with one of the world’s top-ranked hospitals, Gemelli Hospital, and created a dual M.D. program with their associated university, Cattolica University. That furnished a timely signal of what would be coming to his American hospitals, enabling early preparations for one of the gravest threats to public health of the past century.12
The U.S. Centers for Disease Control and Prevention warned of the coronavirus in January, 2020, though relatively few health care providers took much heed at the time, partly because the CDC initially played down the hazards, saying that it “continues to believe the risk” of Covid-19 to the American public “remains low at this time.” Jefferson, however, sounded the alarm, convening an emergency Covid-19 task force on January 28, 2020 with representatives from 28 medical specialties.13
Two days later, the World Health Organization declared a global health emergency. Jefferson advised its 35,000 employees against travel on February 3 and started screening patients for the virus on February 4. It alerted its workforce about a possible catastrophic outbreak, and in an emergency measure more commonly associated with disaster responses to hurricanes and wildfires, it stood-up an incident-command center. On February 10, Jefferson called for crisis preparation by all of the 14 hospitals then in its system.

Informing that mobilization was Jefferson’s footprint in Italy, the first national epicenter for the coronavirus outside of China. Dr. Marino, serving as director of Jefferson’s Italy program called Dr. Guido Bertolaso, a former advisor to the Italian prime minister who had served as a special commissioner for a range of natural calamities in Italy, including earthquakes and volcanoes. Bertolaso had also consulted with the president of Lombardy for Covid-19 emergency planning and he had constructed a hospital on Milan’s fairgrounds dedicated to intensive care for Covid-19 patients.
Jefferson faculty-member Marino asked Bertolaso (who would soon himself become infected with the virus and was later hospitalized but recovered) for guidance from the Italian experience in a conference call on March 18, 2020. What Marino and his colleagues reported from Italy proved to a catalyst for the mobilization of Jefferson in the U.S. In learning that a larger-than-generally expected health crisis seemed imminent, for instance, Jefferson worked to secure a larger-than-normal supply of personal protection equipment.
Since Jefferson had also allied with Italy’s Cattolica University and its teaching hospital near Rome, Marino and his colleagues learned from them how they were managing elective surgeries (they continued operating by dedicating a separate facility to Covid-19 patients) and personnel policies. A faculty member at Cattolica, Dr. Walter Ricciardi, was already consulting with the Italian Minister for Health on the virus emergency, and he shared treatment protocols with Jefferson from his experience on the ground of the Italian epicenter.
In sum, as part of his transformative agenda, Klasko had early broken with the American-centric focus of health-care, not for reasons of net revenue but for global intelligence, providing Jefferson with early warnings that enabled its domestic operations to preemptively respond to the international threat. The early intimations of what was to come provided Klasko’s health system a head-start on risk readiness for the global epidemic.
Redefining Benchmarks
“We can be a 195-year-old academic medical center” but also one that thinks “like a startup,” Klasko insisted. And for that, he believed, fresh benchmarks were essential, a clean break with the past. In taking charge and leading change, Klasko
challenged the criteria by which his medical center had traditionally been judged by others and even by Jefferson itself. He theorized that adherence to traditional criteria pulled Jefferson toward outside goals that were not always consonant with optimizing patient care in a changing environment.
The same for Jefferson’s unhappy tradition of comparing all that it did with a more prestigious neighbor in Philadelphia, the Health System of the University of Pennsylvania. Continuing that contrast would only assure a sense of failure, thought Klasko, since Penn Medicine consistently ranked among the top twenty medical centers in the U.S. “While it might not guarantee success” to abandon that benchmark, he explained, “it was far better than guaranteeing a failure.” A hospital leader should not pick a battle, he told himself, that it was sure to lose.
Klasko also downplayed two benchmarks which had long dominated the national narrative: hospital rankings by US News and World Report and research funding by the National Institutes of Health. He vowed in reports, presentations, and promotions that Jefferson’s evaluative criteria would rely less on those conventions. Still, he took note of the fact that U.S. News and World Report often gave Jefferson high marks for its performance. In 2021, the magazine ranked Jefferson nationally in six adult specialties.14
“Every president before me at Jefferson wanted to compete with Penn,” Klasko explained. But Jefferson was not and would never be Penn, he reasoned, and he thus “didn’t want my goal for the organization to just be a closer ‘second.’” Instead, he “wanted to win a championship” on his own terms. At Jefferson, he decided, it would be innovative education, teamwork assessment, philanthropic giving, and patient services. On the latter two, for instance, he expanded Jefferson’s charitable gifts by more than a factor of two, patient visits by a factor of three, hospital beds by a factor of four, and emergency visits and inpatient days by a factor of five (Table 1). “The natural order of things” was “Penn above Jefferson. But I don’t abide by that.”15
In redefining the institution’s benchmarks, Klasko also pressed his enterprise to embrace emergent technologies for more effective and efficient care, including not just telemedicine but “healthcare at any address.” He built partnerships with outside companies to develop that digital care; he allied with a venture capital firm for digital support of work flows and patient care; and he introduced “design thinking” for sparking innovations in the medical school. Jefferson’s merger with Philadelphia University resulted in a partnership with Princeton University that led to an early design-thinking medical curriculum. Jefferson trained more than 1,500 nurses and physicians to support digital consultations, moving from less than 100 daily telehealth visit in 2019 to nearly 3,000 per day by 2020.16
Leadership Plus
We still need the traditional leadership precepts for presiding over any organization, but we are also wise to gaze well beyond them, whatever the enterprise, as new threats and opportunities call upon managers to add to their long-standing leadership repertoire.
This is the essence of leadership plus: applying what’s always been true for company leaders but at the same time embracing what’s become new. Thinking strategically, deciding decisively, and communicating persuasively remained as vital as ever for Jefferson, but reducing risk and redefining benchmarks had become mission-critical as well.
We have also seen at Jefferson that one individual with a more complete leadership repertoire can indeed move a radical remake into reality while at the same time bringing a team together to sustain the original operations, a dual outcome that established organizations increasingly seek in a more uncertain clime.
The fundamentals of our leadership canon combined with the precepts of maverick leadership are thus what many enterprises are likely to embrace – and in our view should embrace – if they are both to sustain the present enterprise and to prepare it for trying times.
This article was originally published on May 7, 2022.
About the Authors

Stephen K. Klasko, M.D., is Executive in Residence with General Catalyst, Distinguished Fellow for the Digital Economy at the World Economic Forum, and Global Innovation Ambassador for Sheba Medical Center, Israel; and he served as dean of two medical schools and as president of Thomas Jefferson University and CEO of Jefferson Health from 2013 to 2021.

Michael Useem is Faculty Director of the Leadership Center and McNulty Leadership Program of the Wharton School, University of Pennsylvania; and he is author of Investor Capitalism, The Leadership Moment, The Edge: How Ten CEOs Learned to Lead, and The Leader’s Checklist. He offers MBA courses and programs on leadership and governance.
References
- Stephen Klasko was the Chief Executive Officer of Jefferson Health and President of Thomas Jefferson University in 2013-2021, and is now Executive-in-Residence with Catalyst Capital; Michael Useem is Faculty Director of the Leadership Center and McNulty Leadership Program at the Wharton School of the University of Pennsylvania.
- Uncited quotes are from interviews of the second author by the first author.
- Susan Bailey, podcast, May 17, 2021; Centers for Disease Control and Prevention, “Hospitals, Beds, and Occupancy Rates,” https://www.cdc.gov/nchs/data/hus/2017/089.pdf; Harold Brubaker, “Hospital Admissions Continue to Decline, Philadelphia Inquirer, March 14, 2013,
https://www.inquirer.com/philly/business/20130314_Hospital_admissions_continue_to_decline.html. - The Governance Institute, “One Jefferson: Accelerating Reinvention of Academic Medicine through Growth, Integration and Innovation,” 2017; The Governance Institute, “Restructuring Governance for the New Healthcare Environment,” 2020.
- David Binswanger served as the chief executive of a business firm, and William Landman served as a managing partner of an investment company. We conducted the interviews in November, 2021.
- Larry McEvoy, Epidemic Leadership, Wiley, 2021; Karen J. Nichols, Physician Leadership, Wiley, 2021;
- Aaron De Smet, Gerald Lackey, and Leigh M. Weiss, “Untangling Your Organization’s Decision Making,” McKinsey Quarterly, June 21, 2017, www.mckinsey.com/business-functions/organization/our-insights/untangling-your-organizations-decision-making.
- Office of the Chief Financial Officer, Thomas Jefferson University Hospitals Inc., 2022.
- Harold Brubaker, “Split of Jefferson Health System Changes Health-Care Landscape,” Philadelphia Inquirer, March 20, 2014,
https://www.inquirer.com/philly/business/20140321_Split_of_Jefferson_Health_System_changes_health-care_landscape.html; Sharon Oliver, “Health Systems and Hospitals in the Philadelphia Region,”
Philadelphia Business Journal, December 3, 2021,
https://www.bizjournals.com/philadelphia/subscriber-only/2021/12/03/health-systems-and-hospitals-in-the.html. - Harold Brubaker, “FTC Drops Bid to Block Jefferson Move,” Philadelphia Inquirer, March 2, 2021.
- Hermina Ibarra, Act Like a Leader, Think Like a Leader, Harvard Business Review Press, 2015.
- Michael Useem, The Edge: How 10 CEOs Learned to Lead and the Lessons for Us All, PublicAffairs Books, 2021; Howard Kunreuther and Michael Useem, Mastering Catastrophic Risk: How Companies are Coping with Disruption, Oxford University Press, 2018.
- Centers for Disease Control and Prevention, “First Travel-related Case of 2019 Novel Coronavirus Detected in United States,” January 21, 2020, https://www.cdc.gov/media/releases/2020/p0121-novel-coronavirus-travel-case.html.
- US News and World Report, “Jefferson Health-Thomas Jefferson University Hospitals,” 2021, https://health.usnews.com/best-hospitals/area/pa/thomas-jefferson-university-hospital-6230043.
- Advisory Board, “Steve Klasko on Diverging from the Natural Order of Things’ to Move Health Care Forward,” Daily Briefing, November 2, 2021, https://www.advisory.com/daily-briefing/2021/11/02/steve-klasko-interview.
- Laura Dyrda, “’This is Healthcare’s Amazon Moment’: Dr. Stephen Klasko’s 5 Predictions on Healthcare Delivery Post-COVID-19,” Becker’s Hospital Review, April 1, 2020, https://www.beckershospitalreview.com/hospital-management-administration/this-is-healthcare-s-amazon-moment-dr-stephen-klasko-s-5-predictions-on-healthcare-delivery-post-covid-19.html.






